The pelvic floor is the connection between the legs and the trunk. You can imagine how dysfunction here can alter biomechanics up and down the kinetic chain. Let’s dive deeper. Keep scrolling to learn what the pelvic floor is made up of.
Let’s talk anatomy. Everyone has a pelvic floor, (yes, even males!) It consists of multiple layers of muscles that work together to
- Support our organs
- To provide muscular (and sphincter) closure/opening to our urethra and rectum
- Sexual function
- Skeletal structural support
- Pressure management
- Circulation of blood and lymphatic fluid
The layers of muscles
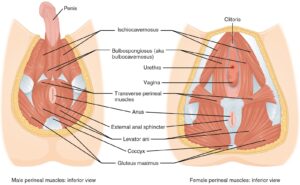
There are 3 muscular “layers” of the pelvic floor, from superficial to deeper muscular structures. Layer 1 includes the Ischiocavernosus, Superficial Transverse Perineum, Bulbocavernosus (Bulbospongiosus in males), and the External Anal Sphincter. These muscles can be palpated externally without need for an internal exam.
Layer 2 muscles include the Urethral Sphincter, Compressor Urethrae, Sphincter Urethrovaginalis, and the Deep Transverse Perineal. These are the muscles that are just inside the pelvic inlet and can be palpated through an internal exam.
Layer 3 muscles include the Levator Ani group (made up of the Pubococcygeus, Puborectalis, and Iliococcygeus), the Coccygeus, Piriformis, and Obturator Internus muscles. Part of the Obturator Internus can be palpated through an external exam, and the Piriformis can be palpated through the glutes externally, but the other muscles can be palapted through an internal exam only.
Fun Fact!
The Obturator Internus muscle attaches from inside the front of the pelvis to the femur (the thigh bone). This muscle plays a role in BOTH pelvic floor AND hip stability. It helps to externally rotate and abduct the hip (move the hip away from midline). As a relatively small muscle, it isn’t a main muscle for moving the hip, and we can think about it as more of an assistant muscle to the Gluteus Maximus, Minimus, and Medius, which are much larger muscles. However if they aren’t doing their jobs, or if they are weaker, the Obturator Internus can kick in and try to help more, and can become overworked and irritated. This can lead to pelvic floor pain, irritation, and difficulty relaxing. Aren’t biomechanics fun?! 😉